

Are you an SLP or SLPA who has a cleft-affected child on your caseload, and you’re not sure how to approach hypernasality and nasal emissions? Or want to learn more about the difference between hypernasality and nasal emissions?
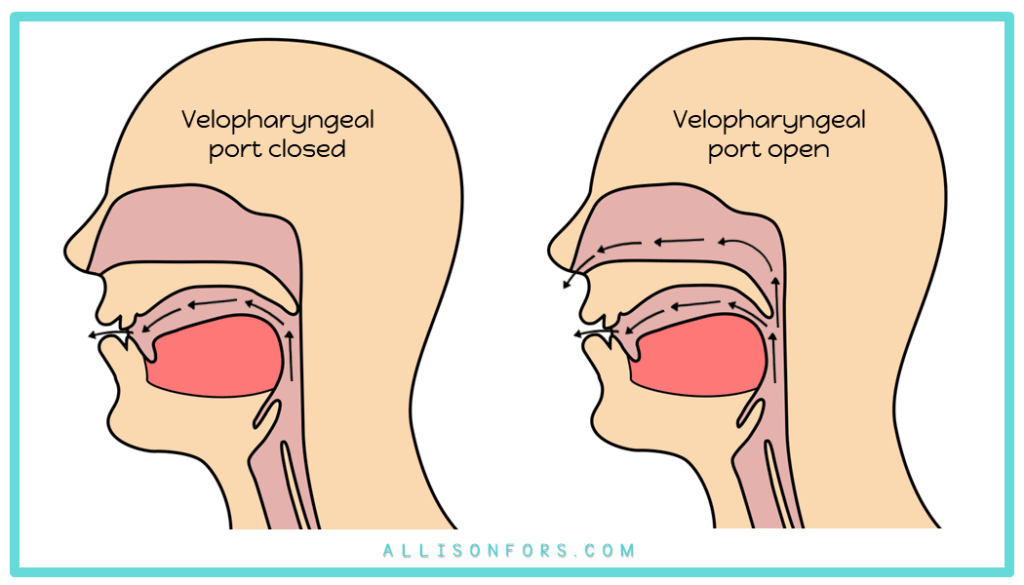
Resonance disorders are common in children with a history of cleft palate. Hypernasality caused by velopharyngeal insufficiency may occur, as well as hyponasality or cul-de-sac resonance caused by changes to structures in the velopharynx or nasal cavity.
Hypernasality occurs when too much sound resonates through the nose. This is the most common resonance disorder. The child may sound like they are talking through their nose, especially on vowels, liquids, glides, and, in severe cases, voiced oral consonants, such as /b, d, g/. High vowels /u, i/ are the most susceptible to hypernasality. Voiced pressure consonants may sound like their nasal cognates: /n/ for /d/ or /m/ for /b/. Hypernasality is typically caused by VPI or a large fistula; it can also occur after adenoidectomy.
Approximately 37% of preschool children with a repaired cleft palate have moderate to severe hypernasality (Hardin-Jones & Jones, 2005).
Surgery is the most common treatment for hypernasal speech due to velopharyngeal insufficiency or fistulas.
Nasal emissions are considered a nasal airflow disorder. Nasal air emission results from an attempt to build up intraoral air pressure to produce consonants. It affects articulation, not resonance, and may occur due to velopharyngeal insufficiency or a fistula. Speech can sound distorted due to extra air escaping through the nasal cavity.
Nasal emissions are audible or inaudible bursts of air through the nose during consonant production. They only occur on consonants, particularly pressure consonants and voiceless sounds (p, b, t, d, k, g, s, z, ch, sh, j). Nasal emission may sound like a snorting, rattling, or blowing sound in the nose. Consonants become weak or omitted. Due to the lack of oral air pressure, the child may use abnormal speech sounds (such as a hard “uh” instead of /g/). Nasal emissions affect articulation, not resonance. They may occur due to velopharyngeal insufficiency or a fistula. Larger velopharyngeal openings may be inaudible.
This requires physical management by a craniofacial team.
Hypernasality is a resonance disorder heard on vowel sounds or voiced plosives. Vowels – especially /u, i/, glides, liquids, and voiced oral consonants are the most affected. Hypernasality does not affect voiceless sounds.
Nasal emission is an airflow disorder heard on oral pressure consonants, especially voiceless consonants. Nasal emissions do not affect vowels or resonance.
When velopharyngeal dysfunction is present, hypernasality and nasal air emission can co-occur.
If the child has true hypernasality or hyponasality from a cleft, then there isn’t much that can be done in therapy. Refer them for a VPI evaluation and likely subsequent scope. Ideally, the child has access to a craniofacial team that they can contact and schedule an appointment with. I highly recommend that they see a craniofacial ENT specialist, rather than a general ENT specialist.
If there are compensatory errors that the child uses to compensate for the structural deficit, then you can address those functional issues while the child undergoes their medical and surgical workup!
It is considered best practice that if the child continues to demonstrate hypernasality or nasal emission after a few months of treatment, they should be referred to a craniofacial specialist.
NASAL AIRFLOW ERRORS CAN BE CATEGORIZED INTO:
Learn more about common compensatory errors, which can be treated through speech therapy.
And learn more about the difference between compensatory errors and obligatory errors.
The Cleft Palate Speech Guidebook is a comprehensive manual for evaluating and treating cleft speech. This unique cleft speech book has concise, easy-to-understand information for SLPs and SLPAs to assess cleft speech. In addition, how to treat articulation and compensatory errors. It contains over 100 pages of accessible information to feel confident in treating cleft speech!

You may also be interested in reading:
Cleft Lip and Palate Topic Page

If you enjoyed this post, please share it!