This page is a compilation of information related to speech intervention in those with cleft lip ± palate. Discover research, ideas, websites, and resources! Bookmark this page or save it to Pinterest with the image at the bottom.
Cleft lip ± palate can co-occur or be independent of one another. A child may also have a submucous cleft, which is oftentimes difficult to detect because the mucous membrane covers the cleft. It is common for children born with a cleft lip ± palate to need speech intervention at some point. Over half of these children will need speech therapy; however, most will develop normal speech by age five.

source: depositphotos.com
Cleft lip repair typically occurs between 3-6 months old and cleft palate repair typically occurs between 8-14 months old.
More surgeries may be needed as a child grows older, such as a pharyngoplasty.
Before palate repair: Babies with cleft palate produce vocalizations as much as babies who are not cleft affected, although they have delayed onset of babbling and first words and they acquire words more slowly. They also prefer words beginning with sonorants (vowels, nasals, liquids, and glides.) This is because these are the sounds they can make without a palate! Encourage /m,n,l,w,j/, “ng”, and vowels, as well as any tongue and lip movement. Some words to model are “me”, “more”, “no”, “mama”, and “wawa” for water, and other approximations. It is important to note that cleft babies are not affected receptively (unless hearing is impacted.) If they are not repeating words back, they are still learning and expanding their vocabulary.
After palate repair: Encourage the use of more sounds /p,b,t,d,k,g,s,z,f/ and target a greater variety of CV, CVC, and CVCV words.
Gather a case history:
Gather concerns:
Conduct an oral mechanism exam:
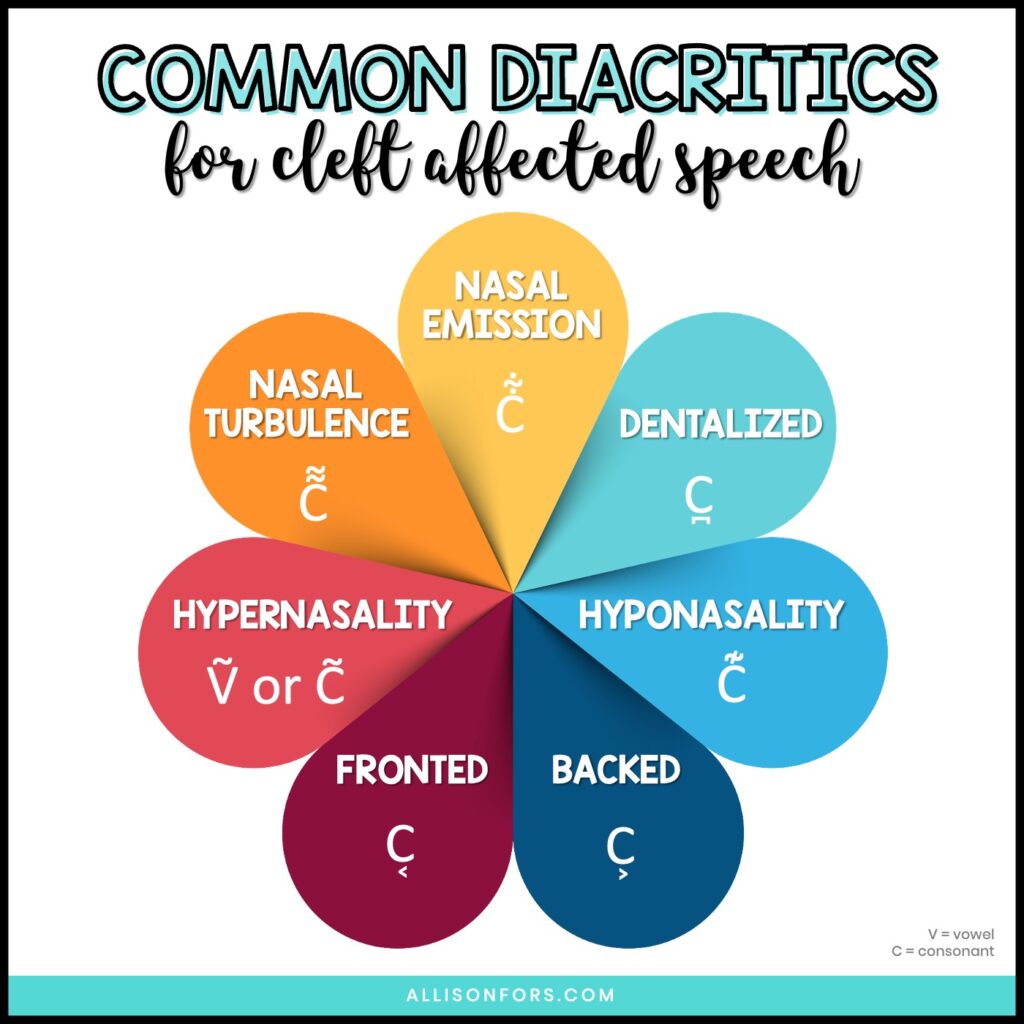
Use phonemically loaded sentences for an informal assessment of overall intelligibility and to access other factors, such as hypernasality and other resonance disorders.
A Guide for Cleft Palate Speech Sampling
You can even get in contact with the craniofacial team’s SLP regarding the child. (Most children are followed by a craniofacial team starting at birth. This includes an SLP, audiologist, dietician, surgeon, dentist, orthodontist, social worker, nurse, and perhaps other professionals.)
A submucous cleft palate is an opening in the muscles of the soft palate, beneath the mucous membrane. These are things to look for in an oral exam, to listen for, and get a history on!

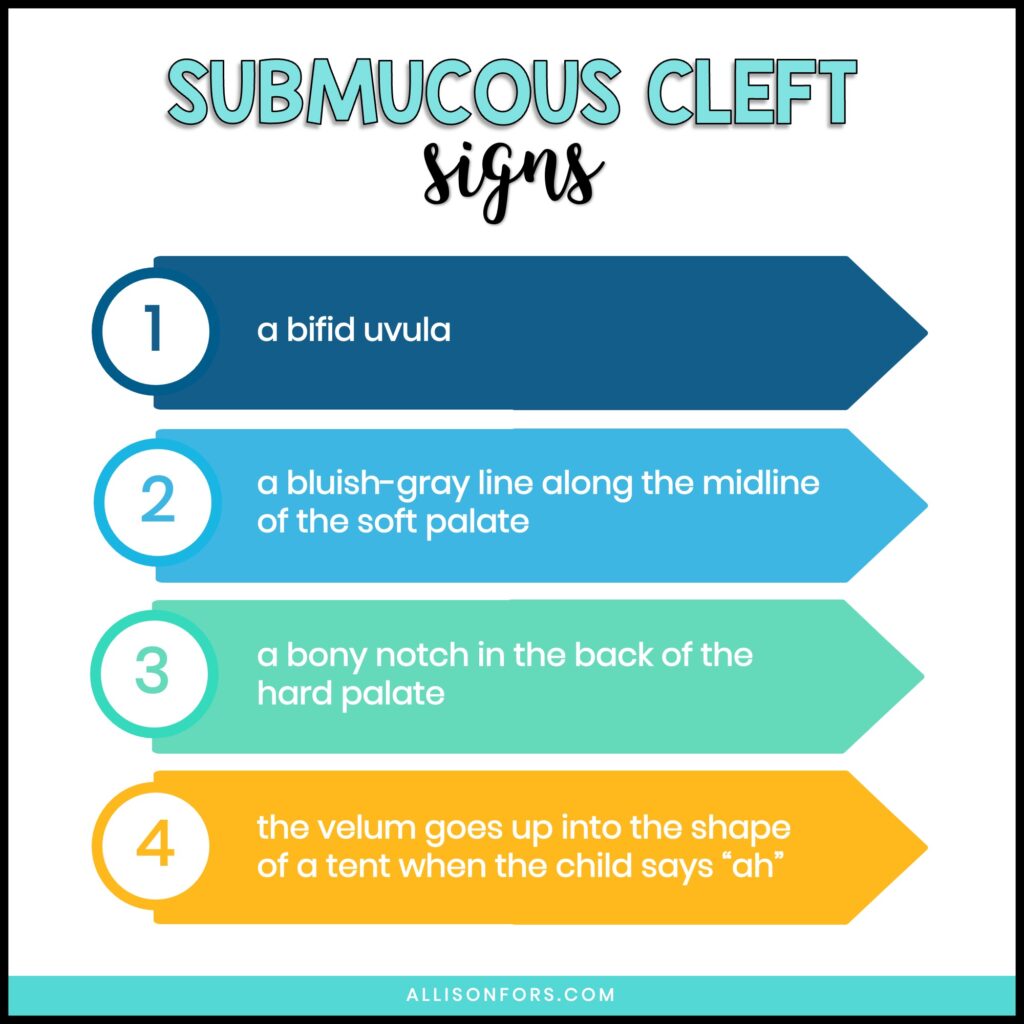
Potential signs:
1. a bifid uvula
2. a bluish-gray line tissue along the midline of the soft palate (this indicates the soft palate muscles are separated)
3. a bony notch in the back of the hard palate
4. the velum goes up into the shape of a tent when the child says “ah”
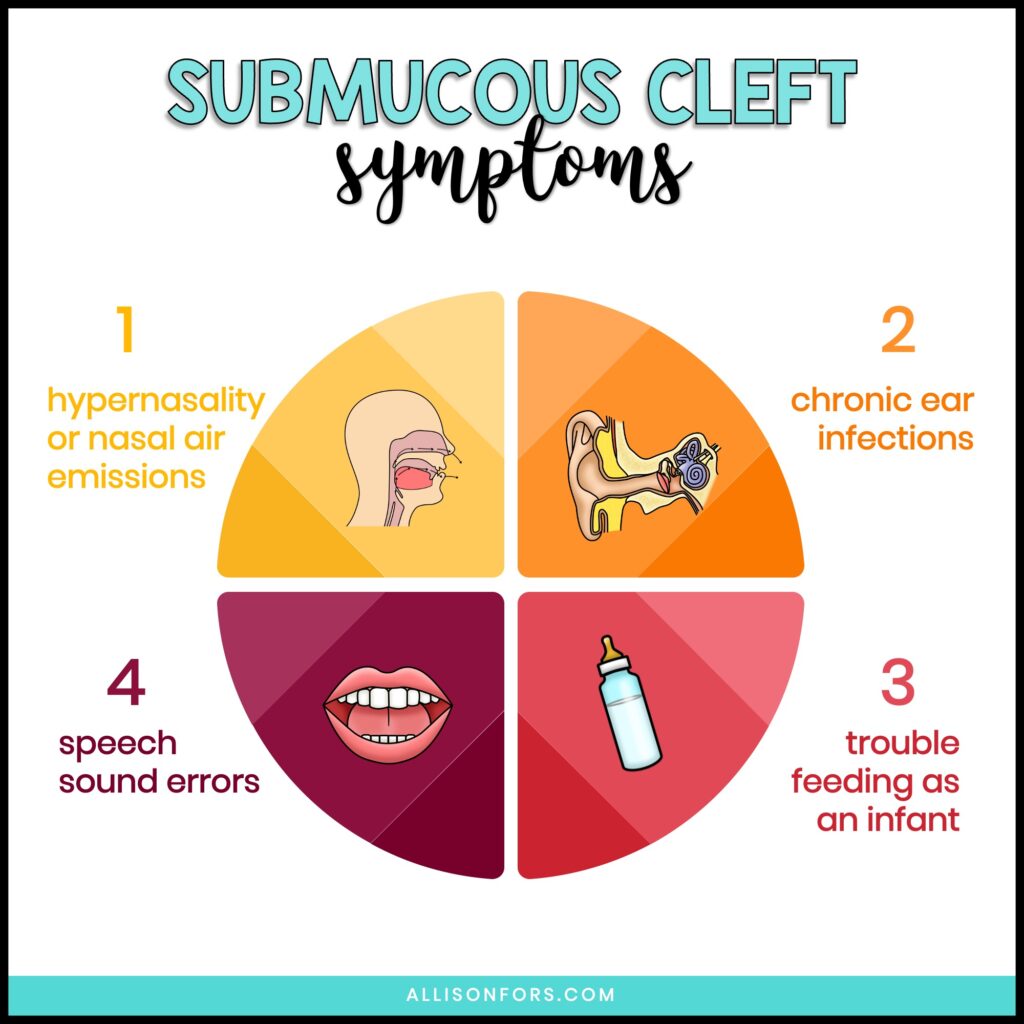
Potential symptoms:
1. hypernasality (“nasally sounding” speech) or nasal air emissions (hearing air leak out the nose during speech)
2. chronic ear infections
3. trouble feeding as an infant (taking a long time to feed, liquid coming through the nose, etc.)
4. speech sound errors
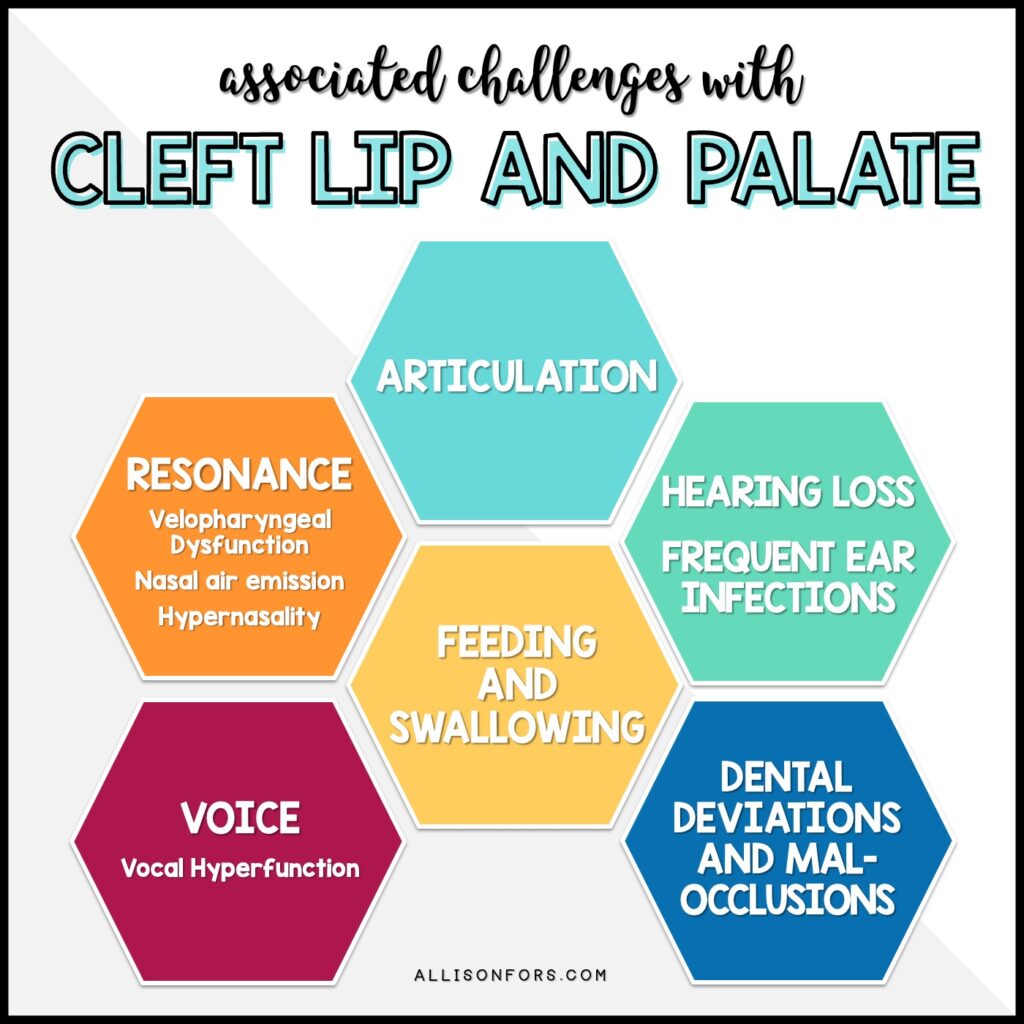
ARTICULATION: A child with a cleft lip may have typical articulation. Those with cleft palates or submucous palates are much more likely to need articulation intervention. Common speech sound errors include glottal stops, nasal fricatives, pharyngeal fricatives, and mid-dorsum palatal stops. Be sure to differentiate between the speech sound errors: obligatory, compensatory, or developmental.
VELOPHARYNGEAL INSUFFICIENCY (VPI): VPI occurs when the velopharyngeal port is not properly closed during speech or swallowing. Air leaks into the nasal passage typically due to the soft palate’s inadequate range of function. This can result in nasal air emission, hypernasality, abnormal speech, and decreased intelligibility. All children with a cleft palate will demonstrate VPI before cleft repair.
NASAL AIR EMISSION: The audible release of bursts of air through the nose during speech.
HYPERNASALITY: A condition when air flows through the nasal passage during voiced consonants and vowels, causing too much nasal resonance.
VOCAL HYPERFUNCTION: A chronic condition when the glottis is overworked resulting in a strained voice, fatigue, or pain.
FEEDING AND SWALLOWING: Children with an isolated cleft lip can use a typical bottle or may be able to breastfeed. Children with a cleft palate oftentimes cannot breastfeed and use a specialty feeder, such as the Dr. Browns Specialty Feeder or Haberman bottle. These bottles don’t require the baby to produce suction and you can pace a baby with the Haberman bottle.
HEARING LOSS: Children with cleft palate are more likely to acquire fluid in the middle ear space and may have frequent ear infections. This can cause mild to moderate hearing loss. Eustachian tube dysfunction is common, and it is present in more than 90% of infants with cleft palates. It can lead to changes in the middle ear and, if left untreated, can cause more permanent hearing loss in adulthood. Some syndromes related to cleft palates have hearing loss associated with them, such as Stickler syndrome. Hearing loss is present in more than 50% of the adult cleft palate population. Those who are hard of hearing tend to remain more hypernasal.
DENTAL DEVIATIONS AND MALOCCLUSIONS: Children with a cleft palate ± lip are more likely to have dental abnormalities. This may include an overbite, underbite, crossbite, extra teeth, missing teeth, and teeth out of alignment. If the alveolar ridge is affected by a cleft, the teeth may be displaced or rotated. These dental differences may affect speech production.
Speech therapy cannot fix hypernasility, hyponasailty, or nasal air emission caused by VPI. However, it is effective in treating abnormal speech sound production (compensatory errors) that were originally caused by VPI.

Children with a cleft palate may learn to use abnormal speech sounds due to abnormal anatomical structures. These speech sounds are called compensatory errors and oftentimes persist after surgery due to learned behavior and require speech therapy to remediate. As SLPs and SLPAs, it is important to recognize and identify specific compensatory errors when working with this population. Approximately 25% of children with cleft palates use compensatory articulation errors and glottal stops are the predominant error!
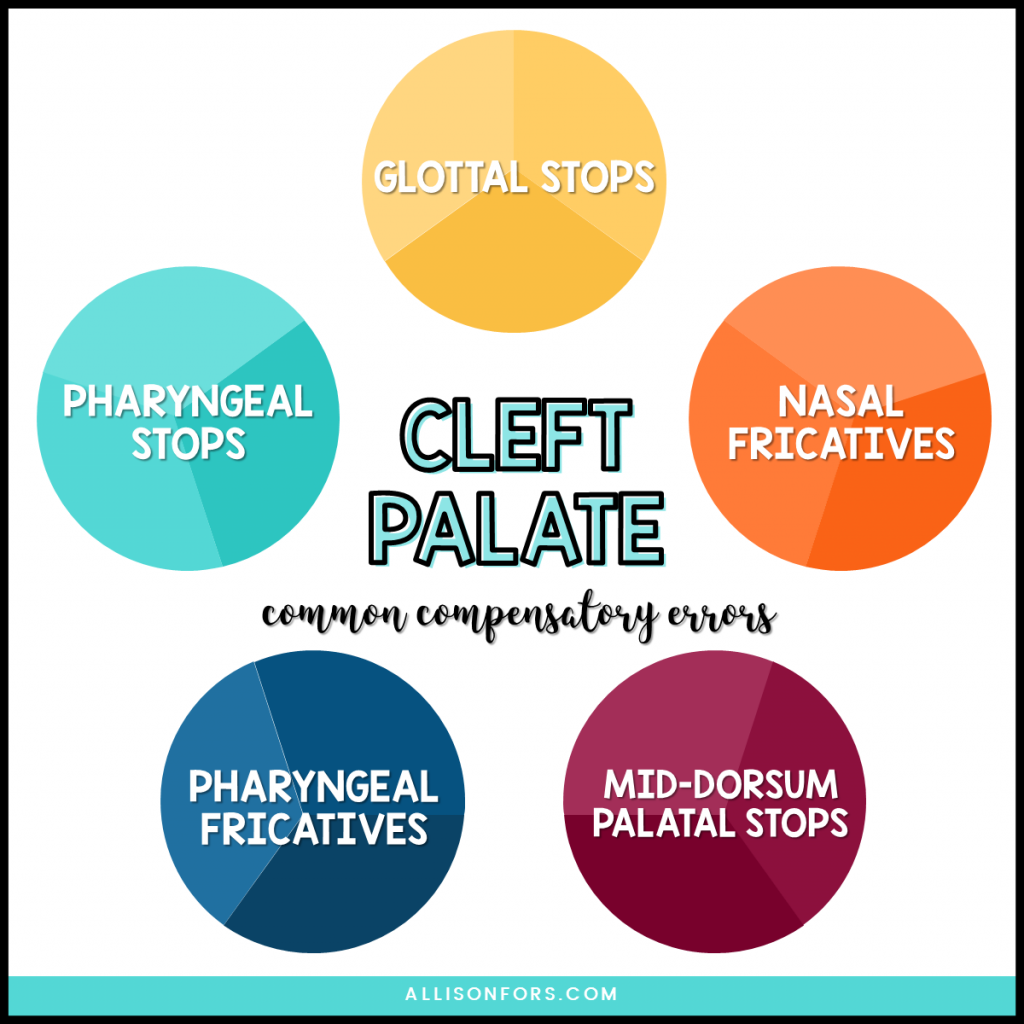
GLOTTAL STOPS: A sound produced by bringing the vocal cords together and then releasing them suddenly instead of the tongue or lips. You may hear or use a glottal stop while producing certain words, such as “button”, instead of fully articulating the “t” in the middle of the word or in “uh oh.” A glottal stop is typically used for /p, b, t, d, k, g/ sounds. For example, a child with a cleft palate may say the word puppy as “uh-ih”.
NASAL FRICATIVES: When air is directed into the nasal cavity while producing a fricative sound such as /f, s, v, z/, “th”, and “sh”.
PHARYNGEAL FRICATIVES: When the wall of the throat is used to produce a fricative sound instead of with the tongue. This is typically used to substitute the /s, z/ and “sh” sounds.
PHARYNGEAL STOPS: When the back of the tongue contacts the wall of the throat to stop airflow. This is typically used to substitute the /k, g/ sounds but may be used for other oral stops or oral pressure consonants.
MID-DORSUM PALATAL STOPS: When airflow is stopped by the tongue contacting the middle of the roof of the mouth and used as a substitute for /t, d, k, g/. This error sounds like a production between a “k” and “t”.
Read more: Common Compensatory Errors
ASHA Clinical Topics: Cleft Lip and Palate
ASHA Clinical Topics: Resonance Disorders
ASHA Evidence Maps: Cleft Lip and Palate Research Articles
ASHA Leader: 10 Common Questions About Cleft/Craniofacial Management Answered
ASHA Leader: Opening the Toolbox for Cleft Palate – Related Speech Disorders
American Cleft Palate-Craniofacial Association
CLAPA – Cleft Lip and Palate Association
Speech Evaluation and Treatment for Patients With Cleft Palate
English Cleft Palate Speech Therapy: Evaluation and Treatment by LeadersProject
Birth to Three – Special Considerations for Speech Sound Disorders in Children with Cleft Palate &/or Velopharyngeal Dysfunction by Anne Bedwinek
Understanding Cleft Lip and Palate by Ann W. Kummer
Speech/Resonance Disorders and Velopharyngeal Dysfunction Part 1 by Ann W. Kummer
Speech/Resonance Disorders and Velopharyngeal Dysfunction Part 2 by Ann W. Kummer
Evaluation of Speech/Resonance Disorders Secondary to Velopharyngeal Dysfunction by Ann W. Kummer
Treatment of Speech/Resonance Disorders Associated With Velopharyngeal Dysfunction by Ann W. Kummer
Dr. Brown’s Feeding Educational Webinars
Upcoming ACPA (American Cleft Palate Craniofacial Association) Webinars
MyFace Webinar: Early Speech & Language Development in Children with Cleft Lip/Palate (free)
Assessment of Speech Sound Disorders in Children with Cleft Palate and/or VPD by Angela Dixon
Advanced Pediatric Feeding Mentorship Group (APFMG): Cleft and Craniofacial Feeding Module
Upcoming and Past ACPA Webinars (Usually only $25 for non-members)
The Clinician’s Guide to Treating Cleft Palate Speech by Peterson-Falzone, Trost-Cardamone, Karnell, and Hardin-Jones (2nd ed.)
Cleft Palate and Craniofacial Anomalies: Effects on Speech and Resonance by Ann Kummer (3rd ed.)
Cleft Palate Speech and Resonance by Vallino, Ruscello, and Zajac (1st ed.)
The Source for Cleft Palate and Craniofacial Speech Disorders by Dr. Linda Vallino
Treating Cleft Palate: Q&A with a Craniofacial SLP
Questions to Ask When Evaluating a Cleft-Affected Child
Tips for Treating Cleft Palate Speech
A Guide to Velopharyngeal Insufficiency
The Connection Between S-Clusters and VPI
Common Cleft Palate Compensatory Errors
Compensatory Errors Versus Obligatory Errors
About Hypernasality and Nasal Emissions
Signs and Symptoms of Submucous Cleft Palate
Cleft Speech Treatment Timeline
How to Help Speech Development Before Palate Repair
A Guide to Oral Mechanism Exams
The Overlooked Connection Between Hearing Loss and Cleft Palate
Children’s Books About Cleft Lip and Palate
Sound Loaded Books for High Pressure Sounds
Cleft and Craniofacial Awareness Month
Listen to a podcast episode where we discuss cleft speech and my personal experiences with a cleft-affected child:
De Facto Leaders – Cleft Palate, Resonance Disorders, and Market Research
SLPs Wine and Cheese – Velopharyngeal Insufficiency
Speechy Things – Hello from the Other Side: Becoming a NICU Mom
The Unexpected Podcast – Cleft Palate

Cleft Palate Speech Guidebook BUNDLE – Your comprehensive guide for evaluation and remediation of cleft palate speech. This cleft speech book has concise, easy-to-understand information for SLPs and SLPAs to assess and treat cleft-affected children.

Assessment of Cleft Palate Speech – Feel confident assessing cleft palate speech, as well as understanding cleft speech development and cleft palate speech characteristics. This unique resource outlines all the information you need to assess a child with cleft lip ± palate. It includes a thorough cleft palate oral mechanism exam, a speech and resonance screener, a cleft case history form, submucous cleft palate speech characteristics, and more.

Treatment of Cleft Palate Speech – A comprehensive manual for information and intervention on treating cleft speech, including compensatory errors, hypernasality, and nasal emissions. This unique resource outlines all the information you need to treat a child with cleft lip ± palate. It includes specific treatment tips, cleft-specific articulation word lists, visuals, and a wide variety of strategies for treating compensatory errors.

Cleft Speech Parent Handouts – 16 parent handouts cover various topics to help the family feel supported in aiding their child’s speech, language, and feeding development.