Learn about hearing loss in children with cleft palate. SLPs need to be aware that ear infections and conductive hearing loss can be a common occurrence in cleft affected infants and children and know how it impacts speech development.
When discussing cleft palate speech, the conversation usually focuses on resonance, velopharyngeal function, and compensatory articulation errors. All those aspects play a critical role, but there’s a piece of the cleft puzzle that doesn’t always get the attention: hearing loss and ear infections.
Children with cleft palate are significantly more prone to hearing difficulties, particularly conductive hearing loss related to chronic middle ear disease. That chronic, often fluctuating hearing loss shapes how these kids process sound, build language, and develop speech.
If a child is inconsistently hearing speech sounds, struggling with fluctuating hearing loss, or missing subtle linguistic information during critical developmental windows, it can affect everything from articulation progress to language comprehension and literacy development.
There is a clear connection between hearing loss and cleft palate. The biggest reason comes down to anatomy and muscle function. Children with a history of cleft palate are more likely to acquire fluid in the middle ear space and may have frequent ear infections.
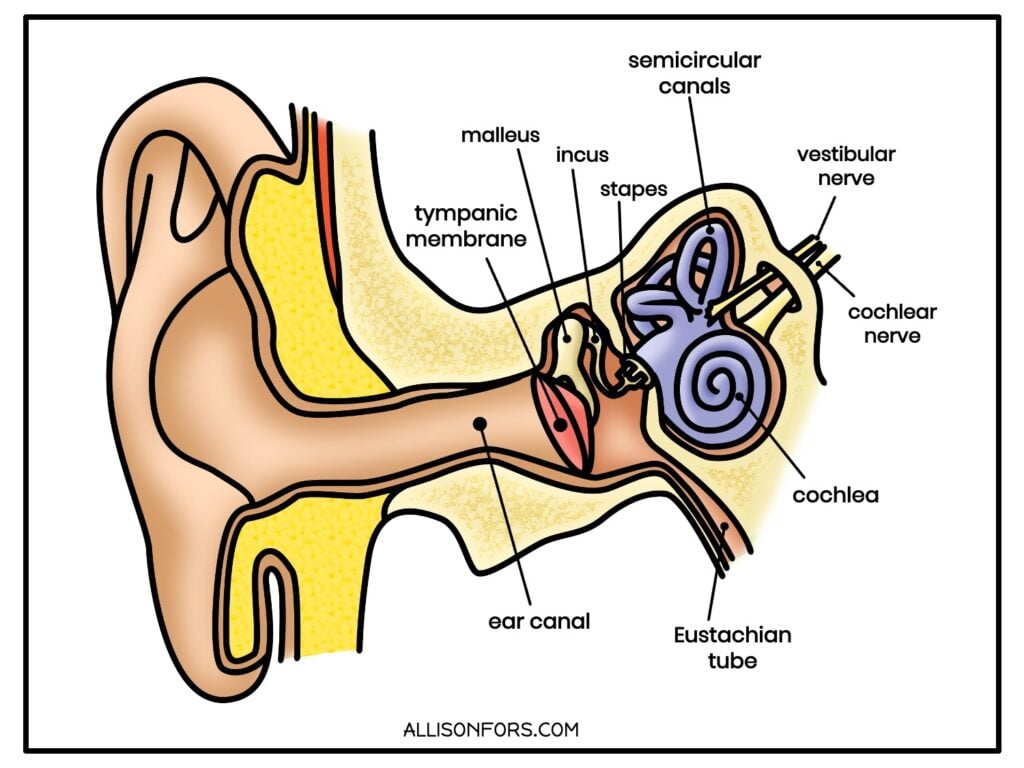
The Eustachian tube connects the middle ear to the back of the throat and helps ventilate the middle ear space. In children with cleft palate, the muscles responsible for opening the Eustachian tube often do not function efficiently because of the structural differences associated with the cleft.
When the Eustachian tube doesn’t open properly, fluid can build up behind the eardrum. This creates an ideal environment for recurrent ear infections and conductive hearing loss. Even after palate repair, many children continue to experience middle ear problems throughout childhood.
Eustachian tube dysfunction is present in more than 90% of infants with cleft palates. It can lead to changes in the middle ear and, if left untreated, cause more permanent hearing loss in adulthood.
This is one of the most common conditions seen in children with cleft palate. OME refers to fluid in the middle ear without signs of acute infection. Sometimes it’s called “silent” fluid because children may not appear sick, but the fluid can still significantly affect hearing.
Hearing loss from OME is typically conductive and may fluctuate over time. One week a child may hear relatively well, and the next week they may struggle to detect softer speech sounds or understand speech in noisy environments.
For SLPs and SLPAs, fluctuating hearing loss can sometimes explain:
Some children experience repeated ear infections with pain, fever, and inflammation. Frequent infections may result in repeated periods of reduced hearing acuity during critical developmental years. Families may become so accustomed to recurrent infections that they don’t always recognize the impact on communication development.
Conductive hearing loss occurs when sound cannot efficiently travel through the outer or middle ear. Unlike sensorineural hearing loss, which involves damage to the inner ear or auditory nerve, conductive hearing loss is caused by a problem transmitting sound through the hearing mechanism itself.
In children with cleft palate, conductive hearing loss is most commonly related to Eustachian tube dysfunction and chronic middle ear fluid (otitis media with effusion). Because the muscles that help open the Eustachian tube do not function efficiently, fluid can become trapped behind the eardrum. This fluid dampens the transmission of sound through the middle ear, resulting in mild-to-moderate hearing loss.
One way to think about it is that the child is hearing through a layer of fluid. Sounds are often muffled, softer, and less distinct than they would be with a healthy, air-filled middle ear.
In children with cleft palate, conductive hearing loss is often temporary or fluctuating as fluid levels change over time. However, repeated episodes can still affect speech and language development, especially during critical learning periods.
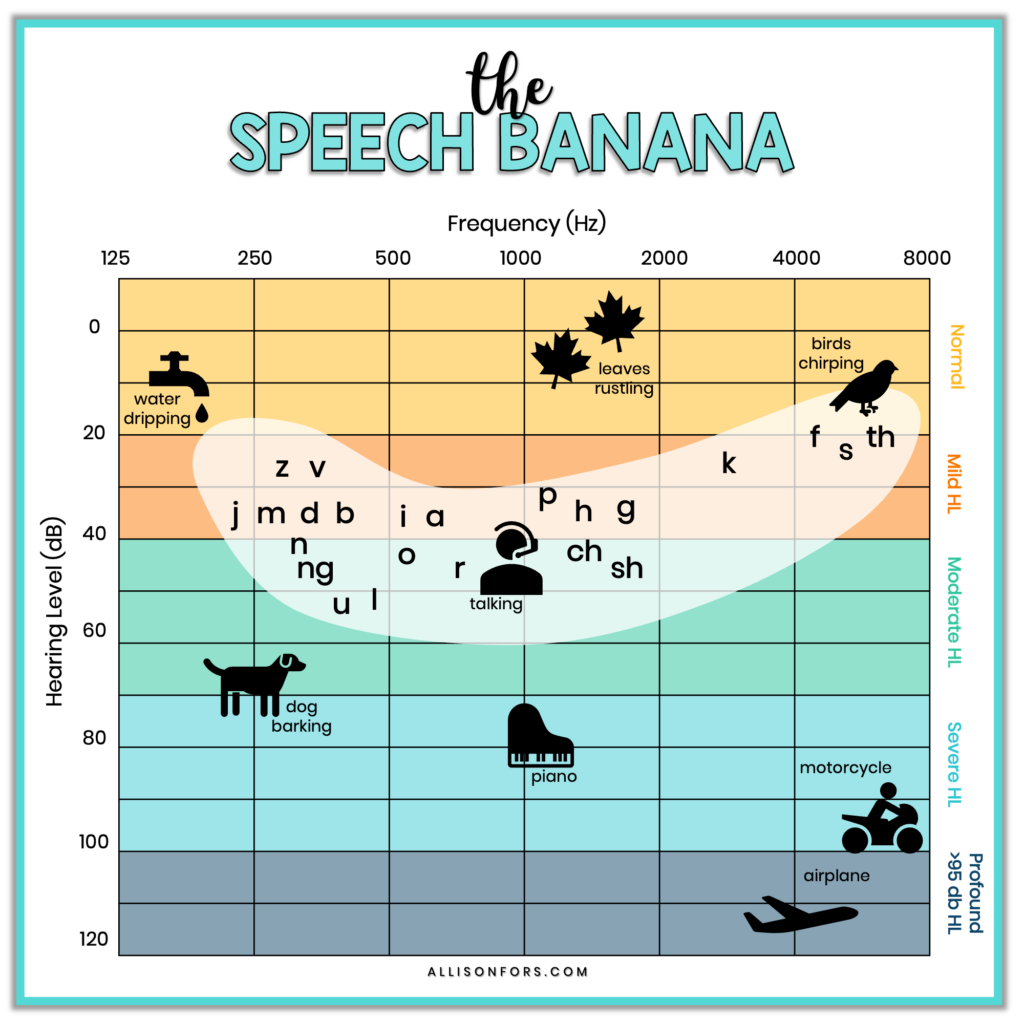
Children do not need to have severe hearing loss for communication to be affected. Missing high-frequency speech sounds such as /f/, /s/, or “th” can influence speech sound acquisition, grammatical markers, phonological awareness, and auditory learning. Even mild hearing loss can reduce consistent access to the speech signal that children rely on to develop communication skills.
The effects of chronic middle ear disease can influence speech development, resonance, language learning, and even the types of articulation errors we observe in therapy. Repeated episodes of mild-to-moderate conductive hearing loss due to OME can cumulatively affect speech and language development over time.
For SLPs, this matters because hearing-related speech characteristics can sometimes look similar to errors associated with cleft palate itself.
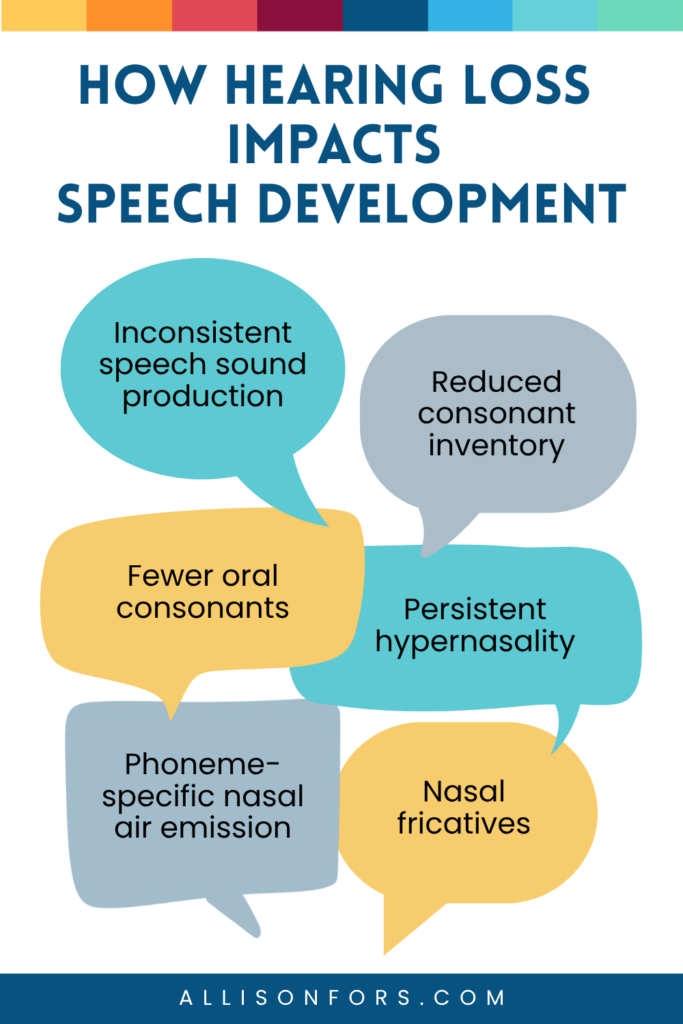
Children with cleft palate and a history of hearing loss have been found to use fewer oral consonants than children with typical hearing (Chapman et al., 2021). A reduced oral consonant inventory can complicate differential diagnosis, making it more difficult to determine whether speech errors are related to velopharyngeal dysfunction, compensatory articulation patterns, or reduced auditory access.
Chronic hearing loss may contribute to:
Hearing loss may also affect resonance and velopharyngeal function. Children who are deaf or hard of hearing are more likely to demonstrate persistent hypernasality, even when structural concerns are not the primary cause.
In some cases, hearing impairment can contribute to velopharyngeal mislearning – speech patterns that resemble velopharyngeal dysfunction despite adequate velopharyngeal anatomy. For example, a child may demonstrate phoneme-specific nasal air emission or hypernasality due to reduced auditory feedback rather than a structural deficit.
SLPs should also be aware of nasal fricatives, a compensatory articulation pattern in which airflow is directed through the nasal cavity during production of fricative sounds such as /s/, /z/, /f/, /v/, “sh,” and “th.” While nasal fricatives are commonly associated with cleft palate, they have also been reported in children with conductive hearing loss and recurrent ear infections.
Similarly, deaf and hard-of-hearing individuals may demonstrate atypical resonance patterns on vowels and nasal consonants. Reduced auditory feedback may affect the timing and coordination of velopharyngeal movements, resulting in speech characteristics that can mimic structural resonance disorders.
If you observe persistent hypernasality, phoneme-specific nasal air emission, nasal fricatives, or an unusually limited oral consonant inventory, hearing history should be part of your differential diagnosis. While structural causes must always be ruled out in children with cleft palate, hearing loss may be a contributing factor that influences both speech production and resonance.
Since hearing loss can directly impact a child’s ability to develop speech and language, ongoing care is necessary. Audiologists should regularly monitor hearing from infancy. ENTs manage middle ear health and tube placement.
Keep in mind that some syndromes that present with a cleft palate are associated with hearing loss. Certain diagnoses bring an elevated risk for hearing loss in children with cleft palate.
22q11.2 Deletion Syndrome: Also called DiGeorge syndrome or velocardiofacial syndrome. Research suggests that approximately 38% of individuals with 22q11.2 deletion syndrome experience hearing impairment, including conductive, sensorineural, and mixed hearing losses (Verheij et al., 2017). This is important because hearing difficulties may not resolve with treatment of middle ear disease alone.
Pierre Robin Sequence (PRS): PRS involves micrognathia, glossoptosis, and typically a wide U-shaped cleft palate, and research shows these children have worse speech outcomes overall compared to kids with isolated cleft palate (Gomez-Meza et al., 2018). The structural picture is more complicated, the Eustachian tube dysfunction tends to be more persistent, and the hearing challenges often stick around longer during the windows when language is being built.
Cleft width also plays a role. Wider clefts have been associated with more severe Eustachian tube dysfunction and higher rates of middle ear pathology, though the relationship is not perfectly linear (Sheahan et al., 2022).

During evaluations and therapy planning, ask families questions such as:
Ideally, children with cleft palate should have audiology monitoring from birth. If you’re picking up a school-aged child with a cleft history and there’s no recent audiological evaluation documented, request their last audiogram or encourage them to get an updated hearing test. If reports are outdated or missing, it may be appropriate to encourage follow-up with the cleft/craniofacial team or pediatrician.
SLPs don’t need to interpret audiograms in depth, but we should feel comfortable identifying:
Children with fluctuating hearing difficulties often struggle more in noisy spaces. Adjust your approach for kids with active hearing loss. Face-to-face positioning, maximizing visual cues, being intentional about room acoustics, and looping in the classroom teacher about seating placement all matter.
Simple supports can help:
If therapy progress seems unusually inconsistent, hearing status should always remain on the radar. A child who suddenly appears less accurate, less attentive, or less responsive may be experiencing another episode of middle ear dysfunction.
Don’t automatically assume speech errors are due to structural or compensatory causes. When you’re seeing an unusual error pattern, hearing should be on your differential. This is especially true with new or emerging nasal fricative substitutions. Research specifically supports referring for audiological evaluation or ENT consult when those appear in a child with cleft palate history (Chapman et al., 2021). A child who’s been getting by with mild hearing loss may produce errors that appear compensatory but actually reflect what they’re not hearing clearly.
Cleft palate speech therapy has a lot of moving parts, and it’s easy for hearing to get pushed aside in favor of the resonance work and articulation goals that feel more concrete. But hearing loss in children with cleft palate is a connection that we cannot afford to overlook. Hearing status, middle ear health, and auditory access all play major roles in communication development and therapy outcomes.
Questions about hearing loss in children with cleft palate?
This page is a compilation of information related to speech intervention in those with cleft lip ± palate. Discover research, ideas, websites, and resources! >> Cleft Speech Information Page
Questions to Ask When Evaluating a Cleft-Affected Child
About Hypernasality and Nasal Emissions
The Cleft Palate Speech Guidebook is a comprehensive manual for evaluating and treating cleft speech, along with parent handouts. This unique cleft speech book has concise, easy-to-understand information for SLPs and SLPAs to assess and treat cleft-affected children. It contains over 100 pages of accessible information to feel confident in treating cleft speech!