

Learn 8 clinical hearing referral red flags that signal a child may need an audiology exam.
Regardless of a child’s medical history, hearing should always be on our radar when assessing and treating speech and language. Educationally significant hearing loss can be unilateral, bilateral, minimal in degree, high frequency, or long-standing conductive – meaning it doesn’t always look the way we expect.
It can be subtle.
It can be fluctuating.
And it can look a lot like a speech or language disorder.
That’s why knowing hearing referral red flags matters for every SLP, regardless of the caseload you serve.
ASHA’s 2023 President Robert Augustine noted that members have seen an increasing number of children with hearing loss that has gone undetected, and that’s not an accident. SLPs spend more structured, observation-rich time with children than most other providers. We’re watching how a child responds to auditory input, how their speech patterns hold up across sessions, and whether their progress matches what we’d expect. That puts speech therapists in a unique position to flag what others may have missed.
The eight indicators below aren’t diagnostic (that’s the audiologist’s job), but these should help you know when a hearing referral is appropriate.
A history of frequent ear infections is one of the most straightforward risk factors to ask about and act on. Chronic or recurring otitis media, especially in young children, creates fluctuating periods of conductive hearing loss that can significantly disrupt early speech and language acquisition.
Ask families directly about a history of ear infections: “Has your child had a lot of ear infections?” Any child with a high frequency of ear infections warrants audiological monitoring, particularly if their speech and language development doesn’t match expectations.
A child who functions reasonably well in a quiet one-on-one setting but struggles in a noisy classroom or therapy room may be managing their hearing loss with context clues.
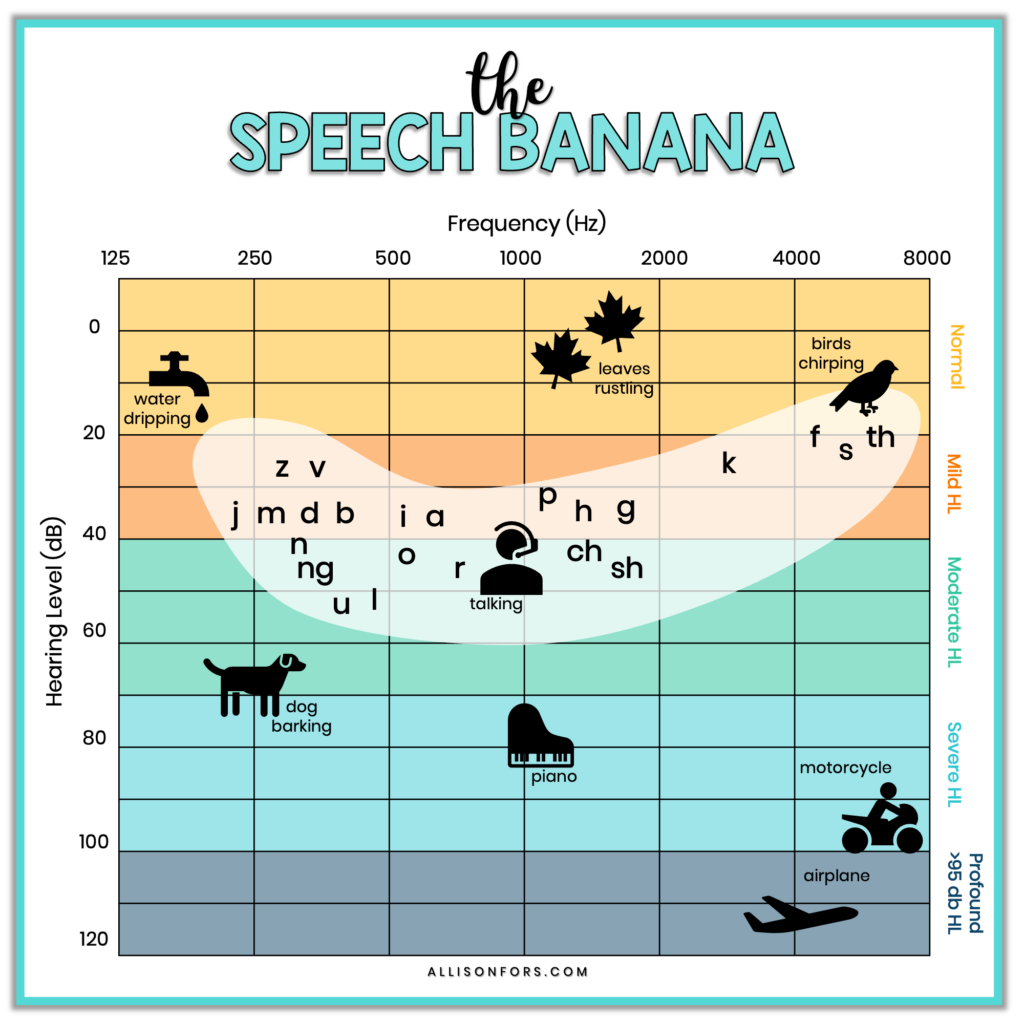
High-frequency consonants such as /s/, /f/, and /t/ are particularly vulnerable to hearing loss, and while audibility may be adequate in quiet conditions, the impact of hearing deficits becomes increasingly critical as background noise increases. If a child seems to track well in your therapy room but teachers report they’re missing instructions, struggling to attend, or frequently asking for repetition in group settings, then a hearing assessment is worth considering.

When a child consistently needs to see your face to respond, or seems to “miss” their name when called from across the room, it’s easy to attribute this to differences in attention, processing, or social communication. And sometimes it is those things. But don’t skip the audiology question first.
Inconsistent or limited access to sound affects the development of spoken language and can also lead to difficulty learning and socializing. A child who has learned to rely on lip reading, proximity, or visual context to compensate for reduced auditory access may look very different in a structured session than they do in the real world. If you’re seeing a reliance on visual cues that seems disproportionate to the child’s other abilities, an audiological evaluation should be considered.
Inconsistency in speech sound production (where the same sound or word is produced correctly one session and not the next, or where accuracy fluctuates in ways that don’t follow a typical phonological pattern) can be one of the harder clinical puzzles to sort out. Before attributing this to motor planning difficulties or inconsistent phonological representations, rule out fluctuating conductive hearing loss.
Inconsistent or limited access to sounds affects the development of spoken language, and when that access is fluctuating (as it often is with OME), the result may appear inconsistent rather than systematically disordered. If a child’s error patterns don’t stabilize across contexts and over time, especially in a child with a history of ear infections, the inconsistency may reflect inconsistent auditory input rather than a processing or motor-based disorder.
A restricted consonant inventory (particularly one dominated by nasals, labials, and low-frequency sounds) is a classic sign of hearing loss in young children. The number of consonants present in the speech of children with hearing impairment is dramatically lower than in typically developing peers.
Specifically, high-frequency consonants like /s/, /f/, /θ/, and /ʃ/ are frequently missing or distorted because they fall in the frequency range most affected by mild-to-moderate hearing loss. If a child’s inventory is limited in ways that don’t fit neatly into a developmental phonological framework, or if they’re older and still missing sounds that should be well-established, hearing should be considered part of the differential.
When a child isn’t making expected progress despite appropriate, evidence-based intervention, we need to ask ourselves what else might be going on. Hearing loss can most definitely be the piece that is missing that you can’t quite pinpoint.
Failure to detect congenital or acquired hearing loss in children may result in lifelong deficits in speech and language acquisition, poor academic performance, personal-social maladjustments, and emotional difficulties. If you’ve adjusted your approach, ruled out other factors, and a child is still not moving, it is good practice to refer the child for an audiological evaluation before assuming the intervention isn’t working. A mild but persistent conductive loss can create enough of an input problem to stall progress.
Nasal fricatives are audible bursts or turbulence through the nose during fricative and affricate production. They are a compensatory error pattern classically associated with velopharyngeal dysfunction. They develop when a child learns to produce airflow through the nasal cavity rather than the oral cavity, often because oral airflow isn’t available or isn’t sufficient.
What’s easy to miss: hearing loss can influence this pattern too. Abnormal nasalization of vowels and nasal consonants in children and adults with hearing loss is related to poor control of the velopharyngeal valve due to the lack of auditory feedback. When auditory feedback is compromised, a child loses one of the key signals needed to regulate oral-nasal airflow balance.
New or worsening nasal fricatives, especially in a child without a known structural explanation, warrant a look. Refer to the cleft/craniofacial team or ENT to evaluate velopharyngeal function, and get an audiology evaluation as well. Don’t assume it’s one or the other.

Hypernasality that doesn’t resolve, doesn’t respond to therapy, or appears without a known structural cause warrants attention. The most common cause of hypernasality is velopharyngeal insufficiency, but hearing loss should also be considered in the differential diagnosis.
Poor control of the velopharyngeal valve, due to a lack of auditory feedback, is related to the duration of the hearing impairment. Children who aren’t receiving accurate auditory feedback may not develop or maintain the motor precision needed for consistent velopharyngeal closure during speech. Hypernasality that persists more than a few months post-surgery should be referred to the cleft palate/craniofacial or velopharyngeal dysfunction team for reassessment. Outside the surgical context, any case of unexplained persistent hypernasality warrants a collaborative workup, with audiology as part of that team.
Did you know that children with a cleft palate are at higher risk for hearing loss? If you work with children who have a history of cleft palate, the connection between cleft palate and hearing loss is not incidental. It’s structural. The levator veli palatini muscle, which plays a key role in Eustachian tube function, is affected by the cleft itself. This means that children with cleft palate universally present with otitis media with effusion, often within the first six months of life.
Routine audiology follow-up should be part of every cleft palate child’s care plan, not a referral made only when someone notices a problem. If you’re seeing children with cleft palate on your caseload who haven’t had a recent hearing evaluation, that’s worth flagging with the family and the broader care team.
Read more about the connection between cleft palate and hearing loss in this post.
Hearing is foundational to everything we do in speech-language pathology. When in doubt, refer. An audiology evaluation is non-invasive, relatively quick, and provides information you cannot get any other way. The earlier a hearing issue is identified and addressed, the better the outcomes, and SLPs are often the best positioned to catch it.
Do you have other hearing referral red flags that you keep an eye out for?
You may also be interested in reading: